|
Introduction
The
occurrence of synovial sarcoma of larynx is
uncommon, accounts for only 8.5% of all sarcomas
in soft tissue, with most cases found in the lower
legs of adolescents.(1) The incidence of this type
of cancer in Cranial -Cervical region is very
uncommon, making up 1% of sarcomas in this area,
and only 10% of those cases are synovial sarcomas.
These tumors typically arise from paravertebral
connective tissue spaces, causing retropharyngeal
or parapharyngeal mass, but can also affect other
areas such as the paranasal sinus, mandible,
parotid, or tonsil.(2) Synovial sarcoma most
commonly affects patients between 20 and 40 years
old and presents with symptoms such as pain,
dyspnea, hoarseness and dysphagia.(3) Synovial
sarcoma does not necessarily arise from the
synovial membrane. Instead, it is believed to
arise from pluripotent mesenchymal cells, which
have the potential to differentiate into various
types of tissues and structures in the body.(4)
Case Report:
A 39 years old male
presented with difficulty in swallowing and change
in voice that had persisted for two months.
Examination revealed a large ulceroproliferative
growth involving the supraglottis, with laryngeal
widening. The patient had a history of transoral
excision of a laryngeal tumor one year prior.

|
| Figure
1: CT scan - Irregular soft tissue mass
involving supraglottis with moderate
heterogenous enhancement |
|
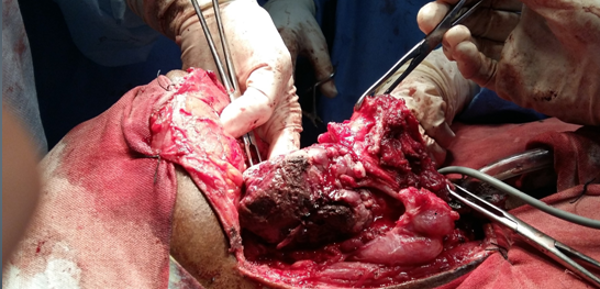
| Figure 2: Intraoperative
findings - Lesion bulging out of PFF,
extending up to cervical vertebra, lesion
filling laryngeal lumen, attached to left
aryepiglottic fold, arytenoid, lateral
pharyngeal wall, superiorly up to
nasopharynx. |
CT scan revealed an
irregular soft tissue mass in the supraglottis
which showed moderate heterogenous
intensification, which was reported as a
hemangiopericytoma of the larynx (Figure 1).
However, intraoperative findings showed a lesion
bulging out of PFF, extending up to the cervical
vertebra, filling the laryngeal lumen, and
attached to the left aryepiglottic fold,
arytenoid, lateral pharyngeal wall, and superiorly
up to the nasopharynx (Figure 2).

|
| Figure
3: Gross revealed laryngeal submucosal
mass with intact mucosa of size 4x4 cm.
|

|
| Figure
4: 4(A) HPE shows Monophasic synovial
sarcoma (10X). 4(B) Spindle cell component
with frequent mitotic activity( 40X) |
Gross examination
revealed a laryngeal submucosal mass of size 4x4
cm occupying the laryngeal lumen and extending up
to the left arytenoid and pharyngeal wall (Figure
3). Upon microscopic examination of biopsy, it was
found that the tumor was arranged in fascicles
composed of spindle cells with scanty cytoplasm,
slightly amphophilic vesicular nuclei with
inconspicuous nucleoli, and numerous mitotic
figures seen (Figure 4). No epithelial component
was observed. Immunohistochemical markers CD99 and
BCl-2 were positive, EMA was focally positive, and
CD34 was negative. With these morphological and
immunohistochemical features monophasic synovial
sarcoma in larynx was diagnosed. Patient underwent
total laryngectomy, partial pharyngectomy, and
pharyngeal reconstruction with PMMC flap. The
postoperative period was uneventful, and the
patient underwent chemotherapy of three cycles .
Discussion:
Synovial sarcoma is
an uncommon cancerous tumor that can occur in any
parts of the body, including the larynx which has
no benign counterpart (5) and is characterized by
a biphasic or monophasic pattern on histological
examination. The biphasic pattern consists of
epitheloid cells arranged in acini,clefts and
stroma with spindle cells, while the monophasic
pattern is mainly composed of spindle cells, which
can sometimes be misdiagnosed as fibrosarcoma.
Synovial sarcomas have poor prognosis. The
survival rate in larynx is not better than in the
extremities. In larynx, 5-year survival rate is
40%.(6)
The symptoms of laryngeal synovial sarcoma include
dysphagia, hoarseness, and shortness of breath on
exertion.(7) The tumor is often located in the
aryepiglottic fold (8-15) and appears as a
submucosal mass, can be pedunculated.
Calcification may also be seen on imaging studies.
To date, there have been only 39 reported cases of
synovial sarcoma occurring in the larynx.(16)
The diagnosis of synovial sarcoma involves a
histological examination, immunohistochemistry,
cytogenetic analysis. A characteristic cytogenetic
finding in synovial sarcoma is the reciprocal
translocation t(X;18)(p11.2;q11.2), which can be
useful in the diagnosis of the monophasic synovial
sarcoma.(12)
The most preferred
treatment for synovial sarcoma in the larynx is
surgery, which involves the complete removal of
the affected tissue with a wide excision and
negative margins being crucial for successful
management. The size of the tumor is a crucial
factor that determines the prognosis, and a larger
tumor size is associated with a worse
outcome.(12,16,17) Postoperative radiotherapy may
be used in head and neck locations, but its
effectiveness on local control and distant
metastasis is not well established. The role of
chemotherapy is also controversial,(8) and its use
may depend on the individual patient and tumor
characteristics.
Post treatment surveillance is crucial for
monitoring recurrence and prolonging disease free
survival. Several years after the initial
diagnosis, distant metastasis can develop, and the
typical cause of death is pulmonary metastasis.
Therefore, close monitoring and surveillance are
necessary to detect any recurrence or metastasis
early and provide appropriate treatment.
Conclusion:
Synovial sarcoma of
the cranio -cervical region is an aggressive
malignancy that should be treated with caution.
Endoscopic surgery with laser ablation is a useful
treatment, and a multidisciplinary approach is
necessary due to the complexity of the tumor. Post
treatment surveillance is crucial for monitoring
recurrence and prolonging disease free survival.
This case report emphasizes the importance of
publishing cases of rare tumors like synovial
sarcoma, as each new case can provide valuable
information on diagnosis and treatment. Therefore,
every case of synovial sarcoma should be published
to contribute to the collective knowledge about
this rare tumor.
Acknowledgment:
Authors wish to thank Dr. Surupa Kurian for her
guidance in this case.
References
- Yadav SD, Anantharamkrishnan D, Kumar D. A
Case of Recurrent Elbow Swelling Turning Out to
Be a Soft Tissue Sarcoma. International
Journal Dental and Medical Sciences.
2022;4(6):317-319.
- Shein G, Sandhu G, Potter A et. al.
Laryngeal synovial sarcoma: A systematic review
of the last 40 years of reported cases. Ear,
Nose and Throat Journal. 2019;100(2).
- Moore DM, Berke GS. Synovial sarcoma of the
head and Neck. Archives of Otolaryngology -
Head and Neck Surgery.
1987;113(3):311–313. .
- Miller LH, Santaella-Latimer L, Miller T.
Synovial sarcoma of the larynx. Trans Am
Acad Ophthalmo Otolaryngol. 1975;80:448-451.
- Geahchan NE, Lambert J, Michau C et al.
Malignant synovioma of the larynx. Ann
Otolaryngol Chir Cervicofac. 1983;100:61-65.
- Pruszczynski M, Manni JJ, Smedts F.
Endolaryngeal Synovial sarcoma: Case report with
Immunohistochemical Studies. Head and Neck.
1989;11(1):76–80. doi:10.1002/hed.2880110113.
- Ferlito A, Caruso G. Endolaryngeal synovial
sarcoma. ORL. 1991;53(2):116–119.
- Danninger R, Humer U, Stammberger H. Synovial
sarcoma, a rare tumour of the larynx (case
report and differential diagnostic
considerations). Laryngo-Rhino-Otol.
1994;73(08):442–444.
- Dei Tos AP, Dal Cin P, Sciot R, Furlanetto A
et al. Synovial sarcoma of the larynx and
hypopharynx. The Annals of Otology,
Rhinology, and Laryngology. 1998
Dec;107(12):1080-5.
- Taylor SM, Ha D, Elluru R et al. Synovial
sarcoma of the pericricoidal soft tissue. Otolaryngol
Head Neck Surg. 2002 Apr;126(4):428-9.
- Papaspyrou S, Kyriakides G, Tapis M.
Endoscopic CO2 Laser Surgery for large synovial
sarcoma of the larynx. Otolaryngol Head
Neck Surg. 2003 Dec;129(6):630-631.
- Skytting BT, Bauer HC, Perfekt R et al. Ki-67
is strongly prognostic in synovial sarcoma:
Analysis based on 86 patients from the
Scandinavian Sarcoma Group Register. British
Journal of Cancer. 1999;80:1809-1814.
- Doval DC, Kannan V, Mukherjee G et al.
Synovial sarcoma of the neck. European
Archives of Oto-Rhino-Laryngology.
1997;254(5):246–250.
|




